At the 32nd Anti-aging Conference in Las Vegas menopause was reviewed, which I call “menopause revisited”. The presenter was Dr. Sara Gottfried who is the director of Precision Medicine. She is also affiliated with the Marcus Institute of Integrative Health, Thomas Jefferson University, Philadelphia, Pennsylvania, US. I am presenting the content of her lecture as the following blog.
Some interesting statistics about menopause
- 1 in 5 women die from either a stroke or a heart attack (this is 7-fold higher than women who die from breast cancer)
- There is general improvement in survival among patients with heart attacks. But women age 35 to 54 have increasing admissions to hospitals with heart attacks
- Women have a 10 to 25% lower chance of early medical care when they come down with a heart attack
- In the US one women dies every 80 seconds from either a heart attack or a stroke
- Menopause starts with the last menstrual period, typically this is between the ages 45 to 55.
- FSH (follicular stimulating hormone) is in the 25.8 and 134.8 mIU/mL range after menopause. The LH (luteinizing hormone) is greater than 15 IU/L.
- There is a small group of women who have premature ovarian deficiency at an age younger than 40. This can be diagnosed by abnormally high values of FSH and LH.
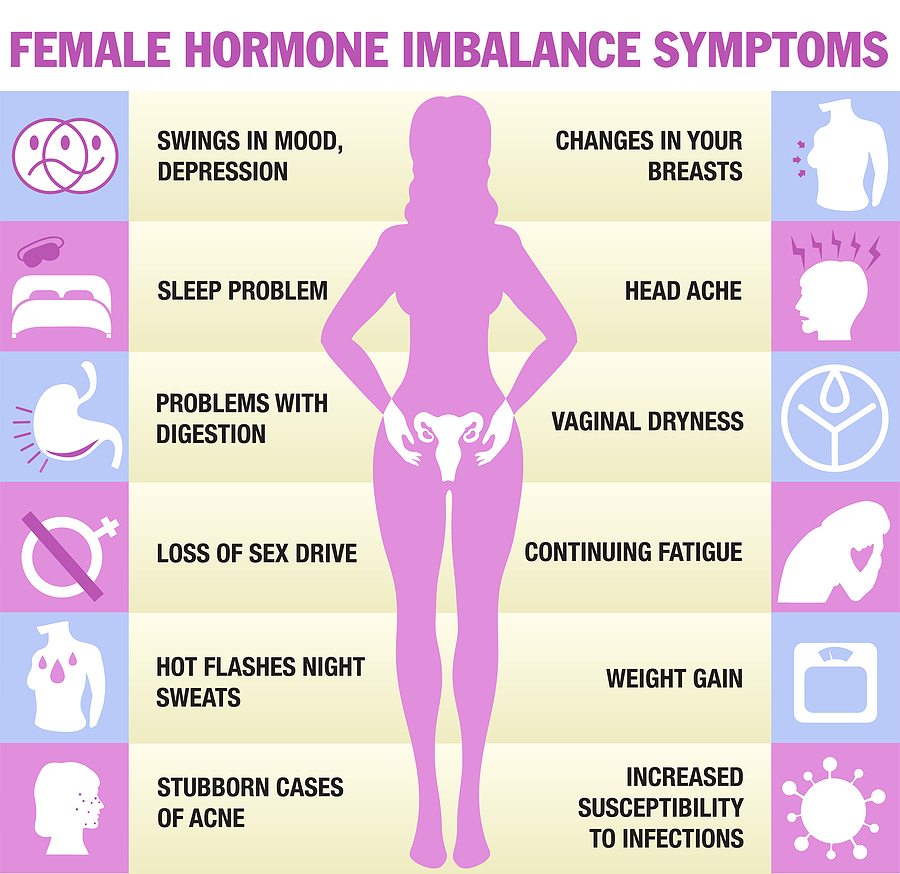
Symptoms of menopause
From age 45 most women do not produce enough estrogen in their ovaries, which leads to the symptoms of menopause. The most common symptoms are: Changes to your periods. Your periods become irregular during perimenopause (the run up to menopause) and then stop altogether. Hot flashes, night sweats, anxiety, low mood, mood swings, brain fog and forgetfulness set in as menopausal symptoms.
Menopause revisited: Hormone derangements
With menopause we know that estrogen production goes down. But when menstruations stop, progesterone production also goes down (lack of ovulation and corpus luteum formation). What physicians did not know until recently is that cortisol production goes up, as measured with morning saliva cortisol levels. It was found recently that morning cortisol levels are 3 times that of normal in postmenopausal women.
Consequences of high cortisol levels
Researchers did MRI scans on postmenopausal women with high cortisol levels and found that there was a reduction of total brain. Their glucose metabolism was prediabetic and their brain had a higher beta-amyloid load. This means that women after menopause are at a higher risk of developing cardiovascular disease (due to a lack of estrogen). But they are also at a higher risk of developing Alzheimer’s disease and diabetes. The lack of progesterone is responsible for emotional problems and depressions. Women age 45 to 55 have a threefold higher suicide rate than men in the same age group.
Menopause revisited: Hormone therapy
Why do postmenopausal women need bioidentical hormone therapy? The physician should treat vasomotor symptoms (hot flashes), mood disturbances, sleep disruption and sexual dysfunction. In addition, he wants to treat cognitive decline, prevent osteoporosis and prolong the healthspan. Healthspan means: staying healthy. Life span does not say anything about the quality of life!
Based on what I said above it is clear that when hormone production suffers or burns out, the only way to rebalance your hormones is to replace them. But physician must be careful: some synthetic hormones, particularly in the treatment of menopause in women can be dangerous to your health (blood clots may develop). For this reason, researchers developed bioidentical hormone replacement where the replacement hormones are identical to the hormones the patient used to produce. This can prolong her life by 10 to 15 years. It is important for the physician to look at all of the hormones in concert as they are all interdependent.
We know for instance that older individuals often are melatonin deficient and this can elevate the morning cortisol level as well. A simple supplement of 3 mg of melatonin at bedtime with a possible repeat during the night when needed will replace missing melatonin production.

Menopause Revisited
Conclusion
It is important that the physician recognizes that in menopause a major hormone derangement will occur. Some patients suffer more than others, but where there is a hormone deficiency, it is necessary to treat the patient with bioidentical hormones. When the physician rebalances her hormone balance properly, the symptoms disappear and the patient feels more energy again. This prevents strokes and heart attacks, diabetes and also Alzheimer’s disease at the same time. The best physicians to treat hormone disbalances in menopause are functional physicians, anti-aging physicians and integrative physicians. But the topic of hormonal deficiency has taken up speed, and some regular general practitioners also have specialized in bioidentical hormone therapy.